Total Anomalous Pulmonary Venous Connection (TAPVC)
What is it?
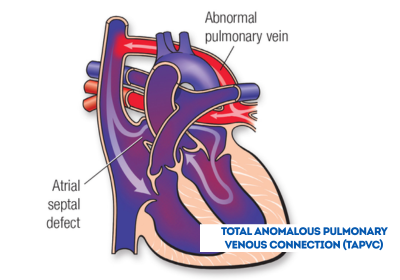
A defect in the veins leading from the lungs to the heart.
In TAPVC, the blood does not take the normal route from the lungs to the heart and out to the body. Instead, the veins from the lungs attach to the heart in abnormal positions and this problem means that oxygenated blood enters or leaks into the wrong chamber.
What causes it?
In most children, the cause isn’t known. Some children can have other heart defects along with TAPVC.
How does it affect the heart?
In the right atrium, oxygen-rich (red) blood from the pulmonary veins mixes with low-oxygen (bluish) blood from the body. Part of this mixture passes through the atrial septum (atrial septal defect) into the left atrium. From there it goes into the left ventricle, then into the aorta and out to the body. The rest of the blood flows through the right ventricle, into the pulmonary artery and on to the lungs. The blood passing through the aorta to the body doesn’t have a normal amount of oxygen, which causes the child to look blue.
How does TAPVC affect my child?
Symptoms may develop soon after birth. In other children, symptoms may be delayed. This partly depends on whether the lung veins are blocked as they drain toward the right atrium. Severe obstruction of the pulmonary veins tends to make infants breathe harder and look bluer (have lower oxygen levels) than infants with little obstruction.
What can be done about the defect?
This defect must be surgically repaired in early infancy. At the time of open-heart surgery, the pulmonary veins are reconnected to the left atrium and the atrial septal defect is closed.
What activities can my child do?
Children with repaired TAPVC may be advised to limit their physical activities to their own endurance. Some competitive sports may have greater risk if there is leftover obstruction in the pulmonary veins, or if the child has heart rhythm problems. Your child’s pediatric cardiologist will help determine the proper level of activity.
What will my child need in the future?
When surgical repair is done in early infancy, the long-term outlook is very good. However, your child will need regular follow-up with a pediatric cardiologist and, once your child reaches adulthood, lifelong regular follow-up with a cardiologist who’s had special training in congenital heart defects. Follow-up is needed to make certain that any remaining problems, such as an obstruction in the pulmonary veins or irregularities in heart rhythm, are treated. Some children may need medicines, heart catheterization or even more surgery.
If my TAPVC was fixed in childhood, what can I expect?
This defect is almost always surgically repaired in early infancy or childhood. At the time of open-heart surgery, the pulmonary veins are reconnected to the left atrium and the atrial septal defect is closed. The prognosis after surgery during childhood is excellent with uncommon late complications. Rarely, obstruction of the pulmonary veins at the site of reconnection can occur. Occasionally abnormal heart rhythms can also occur.
What if the defect is still present? Should it be repaired in adulthood?
It’s rare when the TAPVC hasn’t been repaired in childhood, but most adults in this category are able to have surgery.
Will you need more surgery?
Once the TAPVC has been repaired, it’s unlikely that more surgery will be needed. Rarely, an adult patient may have obstruction that may need to be corrected depending on the severity.
